 2020, Vol. 37
2020, Vol. 37文章信息
- 周笑漪
- ZHOU Xiaoyi
- 葛根芩连汤联合利拉鲁肽对肥胖2型糖尿病湿热困脾证的临床疗效
- Efficacy of Gegen Qinlian Decoction combined with liraglutide in the treatment of obese type 2 diabetes(T2DM) of dampness accumulation in spleen syndrome
- 天津中医药, 2020, 37(12): 1363-1367
- Tianjin Journal of Traditional Chinese Medicine, 2020, 37(12): 1363-1367
- http://dx.doi.org/10.11656/j.issn.1672-1519.2020.12.09
-
文章历史
- 收稿日期: 2020-06-10



2型糖尿病(T2DM)是一个重要的全球公共卫生问题,预计到2035年,将有超过5亿人罹患T2DM[1]。而且,肥胖和超质量糖尿病患者较体质量(W)正常者发生冠心病、脑卒中、心血管疾病的危险性更大,全因病死率更高[2]。因此,对肥胖糖尿病进行治疗时,选择药物需考虑到减质量、增强胰岛素敏感性以及改善血脂等方面的作用[3]。胰高血糖素样肽-1(GLP-1)类似物利拉鲁肽能够以葡萄糖依赖方式促进胰岛素的分泌[4],减慢胃排空和抑制胰高糖素生成[5],从而发挥血糖依赖性的降糖作用,还具有减质量[6]和改善血脂作用[7]。然而,利拉鲁肽减慢胃排空作用常引起明显的厌食、脘腹胀满等胃肠道反应。葛根芩连汤出自张仲景《伤寒论》,多个研究表明,其能够协助西药改善胰岛素敏感性[8-9]和调节血糖。本研究应用葛根芩连汤联合利拉鲁肽,观察其治疗肥胖T2DM证属湿热困脾证患者的疗效。
1 资料和方法 1.1 研究对象选取湖北省中医院2016年10月—2018年10月收治的T2DM合并非酒精性脂肪性肝炎(NAFLD)患者90例。
1.2 纳入标准糖尿病诊断参照2017版《中国2型糖尿病防治指南》的糖尿病诊断标准,肥胖诊断标准按世界卫生组织(WHO)提出的亚洲人W分级标准体重指数(BMI)≥25 kg/m2;中医湿热困脾证诊断参照《中药新药临床研究指导原则》[10]中主症:形体肥胖、脘腹胀满、口渴、食少纳呆、大便溏、舌红苔黄腻;次症:肢体困重、心胸满闷、小便赤黄、脉滑数。主症符合3个或主症2个兼次症2个以上,结合舌脉作出诊断。
1.3 排除标准1)严重心、肝、肾功能不全、感染性疾病、急性心脑血管意外者。2)1型糖尿病、合并急性并发症或3期以上慢性并发症的T2DM患者。3)不满18岁或大于75岁者、孕产妇、合并其他内分泌疾病,如甲状腺疾病、肾上腺疾病、多囊卵巢综合征者。4)对该药物过敏或服用其他影响本研究药物者。
1.4 分组及一般资料将入组者随机平均分为对照组和联合组(通过随机序列数编号,按序号单双分组),每组各45例。试验过程中,无患者脱落。联合组男26例,女19例,年龄(44.2±8.2)岁,病程(12.5±6.4)年;对照组男22例,女23例,年龄(46.1±7.8)岁,病程(11.4±5.4)年。两组性别、年龄及病程长度组间比较采用独立样本t检验,无明显统计学差异(P > 0.05),具有可比性。患者均知情同意,自愿加入该研究。
1.5 方法两组患者均予以糖尿病饮食及运动指导,入组前4周停用影响血脂药物,第1周均给予利拉鲁肽(丹麦诺和诺德公司)0.6 mg每日1次皮下注射,第2周起对照组给予利拉鲁肽1.2 mg每日1次皮下注射;联合组在对照组治疗基础上给予葛根芩连汤口服,方药组成:葛根24 g,黄芩9 g,黄连9 g,甘草6 g。药物由湖北省中医院中药房提供,由湖北省中医院煎药室煎制。每日两次温服,两组均治疗12周。
1.6 观察指标及疗效判定标准两组患者分别于治疗前后测量W、BMI,并于入院24 h内抽取静脉血测定肝功能[血清谷丙转氨酶(ALT)、天门冬氨酸氨基转移酶(AST)、谷氨酰转肽酶(GGT)]、血脂[胆固醇(TC)、三酰甘油(TG)、低密度脂蛋白胆固醇(LDL-C)]、血糖[空腹血糖(FBG)、餐后2 h血糖(2 h PG)]、胰岛素(INS)、糖化血红蛋白(HbA1c),计算HOMA-IR值(FBG×空腹INS/22.5)。其中血糖、血脂、肝功能采用日立7600型全自动生化分析仪测定、胰岛素采用全自动免疫分析仪测定、HbA1c采用离子交换层析法测定。同时进行中医症状评分。按照《中药新药临床研究指导原则》湿热困脾证,针对脘腹胀满、食少腹胀、便溏不爽、心胸满闷、肢体困重、舌红苔黄腻及脉滑数6项进行症候评分,按无、轻度、中度、重度分别记为0、2、4、6分,分值高代表程度重。
1.7 统计学方法采用SPSS 23.0统计软件处理数据,计量资料采用(x±s)表示,组内比较采用配对t检验,组间比较采用独立样本t检验。计数资料用构成比或率表示,组间比较采用χ2检验,P < 0.05为差异具有统计学意义。
2 结果 2.1 两组治疗前后W、BMI、HOMA-IR、肝功能比较两组治疗前W、BMI、HOMA-IR、ALT、AST、GGT比较差异无统计学意义(P > 0.05),治疗后两组指标较治疗前均显著改善(P < 0.05),联合组与对照组比较HOMA-IR改善程度更优(P < 0.05),而W、BMI、肝功能与对照组改善程度差异无统计学意义(P > 0.05),见表 1。

|
治疗前两组FBG、2 h BG、HbA1c、TC、TG及LDL-C比较差异无统计学意义(P > 0.05),治疗后两组血糖、HbA1c及血脂均显著改善(P < 0.05),且治疗后联合组FBG、2 h BG、HbA1c、TC、TG及LDL-C改善情况优于对照组(P < 0.05),见表 2。

|
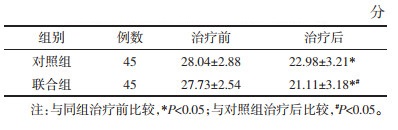
治疗前两组的中医症状积分无统计学意义(P > 0.05),治疗后两组中医症状积分均较治疗前显著降低(P < 0.05),而联合组中医症状积分显著优于对照组(P < 0.05),见表 3。
|
对照组治疗中有3例患者出现恶心伴随腹泻,5例厌食,均可耐受,4周后缓解。联合组出现2例厌食。两组均未观察到低血糖反应。两组不良反应有统计学差异(χ2=4.050,P=0.044 < 0.05)。
3 讨论T2DM与肥胖关系密切。肥胖使游离脂肪酸和葡萄糖增加,导致胰岛素分泌增加,且肝脏、肾脏、肌肉等组织对胰岛素清除能力下降而导致高胰岛素血症[11]。此外,肥胖者胰岛素抑制肝糖输出作用下降、促进脂肪和肌肉利用葡萄糖能力受损,对胰岛素作用产生抵抗[12],而伴随肥胖而来的血脂异常会加重胰岛素抵抗[13]。
GLP-1是一种肠促胰岛素激素,可增加胰岛素分泌[4],抑制胰高糖素分泌并减慢胃排空[5],但半衰期短,进入循环后马上被DPP4酶降解。利拉鲁肽性质稳定,与GLP-1有97%序列一致,具有良好降糖有效性和安全性[14],且具有显著减质量作用[15]。研究发现利拉鲁肽具有降低肝糖生成,改善肝脏胰岛素抵抗,减少外周脂肪分解,降低游离脂肪酸浓度的作用[16]。然而,利拉鲁肽的胃肠道不良反应较为显著,其可能的机制为利拉鲁肽减慢胃排空而导致胃扩张,引起恶心和厌食,不良反应常在药物增加剂量时发生[17],易导致患者依从性下降。
T2DM属中医“消渴”范畴,现代人由于多食少动,喜食肥甘,昼夜颠倒,导致脾失运化,湿聚困脾,《名医指掌》云:“人惟酒色是耽,嗜食辛辣浓味……而三消之病生焉”,湿热困脾证为消渴常见证型[18]。葛根芩连汤源自《伤寒论》,原用以治疗湿热所致腹泻,但古代医家即对其应用范围进行了扩大,陆九芝云“葛根芩连一方独见遗于阳明者……孰不知此方之所用者宏,而所包者广也”。近年来,对于葛根芩连汤用于糖尿病,特别是湿热证的疗效甚佳。多个研究发现葛根芩连汤具有保护β细胞,改善胰岛素敏感性的作用[19-20]。对动物模型的研究发现,葛根芩连汤可通过抑制炎症因子释放[21]、激活过氧化物酶体增殖物激活受体γ上调脂联素和葡萄糖转运蛋白4来调节糖代谢,改善脂肪组织胰岛素抵抗[22]。方中葛根的主要成分葛根素能通过减轻氧化应激损伤,保护端粒长度来抑制β细胞凋亡,同时还可阻止蛋白质糖基化进程、减少糖基化终末产物的生成,从而降低血糖[23];黄芩的主要有效成分黄芩苷能通过激活P38MAPK/PGC-1α/GLUT4和AKT/AS160/GLUT4信号通路改善胰岛素抵抗[24];黄连的有效成分小檗碱能抑制肿瘤坏死因子-α(TNF-α)及游离脂肪酸(FFA)的表达,改善胰岛素抵抗[25],并同时具有改善血脂及抗炎作用[26]。先贤有云,“药有个性之特长,方有合群之妙用”,葛根芩连汤方中,葛根为君药,归肺胃经,生津止渴,升阳止泻,黄连黄芩为臣药,黄连清胃肠湿热,黄芩兼能清肺胃实热。甘草和中调味,顾护脾胃,兼可生津。全方共奏清热燥湿、醒脾生津之功效。
本研究应用葛根芩连汤联合利拉鲁肽治疗肥胖2型糖尿病,在改善W、BMI和肝功能方面与利拉鲁肽单药效果相当,但对于血糖、HbA1c、HOMA-IR、血脂和中医症状积分的改善显著优于利拉鲁肽单药,对照组出现3例恶心伴腹泻,5例厌食,而联合组出现2例厌食,不良反应显著低于对照组。由此推断葛根芩连汤不仅能协同利拉鲁肽发挥改善胰岛素敏感性、降低血糖和调节血脂的作用,而且能显著改善临床症状和减轻利拉鲁肽的胃肠道不良反应。
综上所述,葛根芩连汤联合利拉鲁肽治疗肥胖T2DM湿热困脾证患者比单用利拉鲁肽疗效更好,可以更显著改善血糖、HbA1c、HOMA-IR、血脂和中医症状积分在内的多项指标,而且能显著降低利拉鲁肽引起的胃肠道不良反应,值得临床推广。
| [1] |
GUARIGUAT A L, WHITING D R, HAMBLETON I, et al. Global estimates of diabetes prevalence for 2013 and projections for 2035[J]. Diabetes Research & Clinical Practice, 2014, 103(2): 137-149. |
| [2] |
LIU X M, LIU Y J, ZHAN J, et al. Overweight, obesity and risk of all-cause and cardiovascular mortality in patients with type 2 diabetes mellitus:a dose-response meta-analysis of prospective cohort studies[J]. European Journal of Epidemiology, 2015, 30(1): 35-45. DOI:10.1007/s10654-014-9973-5 |
| [3] |
YANDRAPALL I S, ARONOW W S, SARAIVA F K, et al. Prevalence of obesity in type 2 diabetes in secondary care:association with cardiovascular risk factors[J]. Diabetes Care, 2015, 9(3): 753-767. |
| [4] |
ORSKOV C, WETTERGREN A, HOLST J J. Secretion of the incretin hormones glucagon-like peptide-1 and gastric inhibitory polypeptide correlates with insulin secretion in normal man throughout the day[J]. Scandinavian Journal of Gastroenterology, 1996, 31(7): 665-670. DOI:10.3109/00365529609009147 |
| [5] |
WETTERGREN A, SCHIOLDAGER B, MORTENSEN P E, et al. Truncated GLP-1(proglucagon 78-107-amide) inhibits gastric and pancreatic functions in man[J]. Digestive Diseases and Sciences, 1993, 38(4): 665-673. DOI:10.1007/BF01316798 |
| [6] |
NUFFER W A, TRUJILLO J M. Liraglutide:A New Option for the treatment of obesity[J]. Pharmacotherapy, 2015, 35(10): 926-934. DOI:10.1002/phar.1639 |
| [7] |
ARMSTRONG M J, HOULIHAN D D, ROWE I A, et al. Safety and efficacy of liraglutide in patients with type 2 diabetes and elevated liver enzymes:individual patient data meta-analysis of the LEAD program[J]. Alimentary Pharmacology & Therapeutics, 2013, 37(2): 234-242. |
| [8] |
葛爱利. 葛根芩连汤对湿热型2型糖尿病患者胰岛素抵抗的影响[J]. 北方药学, 2018, 15(11): 43-44. GE A L. The affection of Gegen Qinlian Decoction on the insulin resistance of type 2 diabetes of damp-heat type[J]. Journal of North Pharmacy, 2018, 15(11): 43-44. DOI:10.3969/j.issn.1672-8351.2018.11.033 |
| [9] |
章常华, 孙军, 肖琴, 等. 葛根芩连汤含药血清对L6肌细胞胰岛素抵抗模型中PI3K、Akt、GLUT4、AMPK蛋白的影响[J]. 时珍国医国药, 2018, 29(7): 1537-1540. ZHANG C H, SUN J, XIAO Q, et al. Effects of Gegenqinlian Decoction-containing serum on PI3K, Akt, GLUT4 and AMPK proteins in insulin resistance model of L6 skeletal muscle cells[J]. Lishizhen Medicine and Materia Medica Research, 2018, 29(7): 1537-1540. |
| [10] |
国家中医药管理局.中药新药临床研究指导原则[S].北京: 中国医药科技出版社, 2002: 367-368. National Administration of Traditional Chinese Medicine. Guideline for clinical trials of new patent Chinese Medicines[S].Beijing: China Medical Science Press, 2002: 367-368. |
| [11] |
STEAR S A, O'RAHILLY S, SEMPLE R K, et al. Metabolic insights from extreme human insulin resistance phenotypes[J]. Best Practice Research Clinical Endocrinology Metabolism, 2012, 26(2): 145-157. DOI:10.1016/j.beem.2011.09.003 |
| [12] |
SALTIEL A R, KAHN C R. Insulin signalling and the regulation of glucose and lipid metabolism[J]. Nature, 2001, 414(6865): 799-806. DOI:10.1038/414799a |
| [13] |
TENENBAU M A, KLEMPFNER R, FISMAN E Z. Hypertriglyceridemia:a too long unfairly neglected major cardiovascular risk factor[J]. Cardiovascular Diabetology, 2014, 13(1): 159. DOI:10.1186/s12933-014-0159-y |
| [14] |
王雅清. 利拉鲁肽联合二甲双胍治疗2型糖尿病临床疗效和安全性评估分析[J]. 河北医药, 2019, 41(3): 392-395. WANG Y Q. The clinical efficacy and safety assessment of liraglutide combined with metformin in treatment of type 2 diabetes mellitus[J]. Hebei Medical Journal, 2019, 41(3): 392-395. |
| [15] |
FUJIOK A K, O'NEIL P M, DAVIES M, et al. Early weight loss with liraglutide 3.0 mg predicts 1-year weight loss and is associated with improvements in clinical markers[J]. Obesity (Silver Spring), 2016, 24(11): 2278-2288. DOI:10.1002/oby.21629 |
| [16] |
ARMSTRONG M J, GAUNT P, AITHAL G P, et al. Liraglutide safety and efficacy in patients with non-alcoholic steatohepatitis(LEAN):amulticentre, double-blind, randomized, placebo-controlled phase 2 study[J]. Lancet, 2016, 387(10019): 679-690. DOI:10.1016/S0140-6736(15)00803-X |
| [17] |
潘长玉. 长效人胰升血糖素样肽-1类似物利拉鲁肽的安全性回顾[J]. 中国糖尿病杂志, 2011, 19(7): 555-558. PAN C Y. The review on safety of the human long-acting GLP-1 analogue, liraglutide[J]. Chinese Journal of Diabetes, 2011, 19(7): 555-558. |
| [18] |
钱玲玲, 陈晓. 2型糖尿病中医证型与胰岛素样生长因子-1、Homa-IR指数关系研究[J]. 四川中医, 2018, 36(7): 86-89. QIAN L L, CHEN X. Relation Research Between Traditional Chinese Medicine syndrome type of type 2 diabetes mellitus and insulin-like growth factor-Ⅰ, Homa-IR index[J]. Journal of Sichuan Traditional Chinese Medicine, 2018, 36(7): 86-89. |
| [19] |
周琦, 朱向东, 仝小林, 等. 葛根芩连汤对2型糖尿病模型大鼠胰岛细胞IRS-2/PI3K-Akt通路的影响[J]. 中医杂志, 2018, 59(11): 973-977. ZHOU Q, ZHU X D, TONG X L, et al. Effect of GegenQinlian Decoction on IRS-2/PI3K-Akt pathway in islet cells of type 2 diabetes model rats[J]. Journal of Traditional Chinese Medicine, 2018, 59(11): 973-977. |
| [20] |
刘亮. 葛根芩连汤对糖尿病大鼠早期视网膜病变影响的实验研究[J]. 天津中医药, 2016, 33(7): 425-429. LIU L. Experimental study of GegenQinlian Tang on the impact of early retinopathy in diabetic rats[J]. Tianjin Journal of Traditional Chinese Medicine, 2016, 33(7): 425-429. |
| [21] |
闫忠红, 刘勇, 刘硕, 等. 葛根芩连汤对2型糖尿病大鼠胰岛素抵抗及炎性因子的影响[J]. 长春中医药大学学报, 2019, 35(4): 720-723. YAN Z H, LIU Y, LIU S, et al. Effect of GegenQinlian Decoction on insulin resistance and inflammatory factors in type 2 diabetes mellitus rats[J]. Journal of Changchun University of Traditional Chinese Medicine, 2019, 35(4): 720-723. |
| [22] |
罗新新, 朱水兰, 李冰涛, 等. 葛根芩连汤激活PPARγ上调脂联素和GLUT4表达改善脂肪胰岛素抵抗[J]. 中国中药杂志, 2017, 42(23): 4641-4648. LUO X X, ZHU S L, LI B T, et al. Gegen Qinlian Decoction activates PPARγ to ameliorate adipocytic insulin resistance in diabetic SD rats and IR-3T3-L1 adipocytes[J]. China Journal of Chinese Materia Medica, 2017, 42(23): 4641-4648. |
| [23] |
袁媛, 侯雪峰, 封亮, 等. 葛根素对体内外晚期糖基化终末产物形成的抑制作用[J]. 中草药, 2017, 48(7): 1386-1390. YUAN Y, HOU X F, FENG L, et al. Inhibition of puerarin on formation of advanced glycation end products in vivo and in vitro[J]. Chinese Traditional and Herbal Drugs, 2017, 48(7): 1386-1390. |
| [24] |
方彭华.基于GALR2/GLUT4信号通路探讨黄芩苷干预胰岛素抵抗的作用及机制[D].扬州: 扬州大学, 2017. FANG P H. To explore regulative mechanism and effects of baicalin on insulin resistance through GALR2/GLUT4 pathway[D].Yangzhou: Yangzhou University, 2017. |
| [25] |
黄娟, 胡维, 林湘东. 盐酸小檗碱对2型糖尿病胰岛素抵抗的改善作用及其机制[J]. 中国老年学杂志, 2018, 38(17): 4130-4132. HUANG J, HU W, LIN X D, et al. Improvement of insulin resistance in type 2 diabetes mellitus by berberine hydrochloride and its mechanism[J]. Chinese Journal of Gerontology, 2018, 38(17): 4130-4132. DOI:10.3969/j.issn.1005-9202.2018.17.013 |
| [26] |
任妍林, 王定坤, 董慧, 等. 小檗碱治疗糖尿病肾病的研究进展[J]. 中国中药杂志, 2017, 42(3): 438-442. REN Y L, WANG D K, DONG H, et al. Research progress of berberine in treatment of diabetic kidney disease[J]. China Journal of Chinese Materia Medica, 2017, 42(3): 438-442. |