 2021, Vol. 38
2021, Vol. 38文章信息
- 姚鹏, 康洪昌, 王江, 郭乾坤, 李明越, 蔡宝琪, 冯璐
- YAO Peng, KANG Hongchang, WANG Jiang, GUO Qiankun, LI Mingyue, CAI Baoqi, FENG Lu
- 荜铃胃痛颗粒联合三联疗法治疗慢性萎缩性胃炎合并幽门螺杆菌感染的临床研究
- The clinical efficacy of Biling Weitong Granules combined with triple therapy in the treatment of chronic atrophic gastritis complicated with helicobacter pylori infection
- 天津中医药, 2021, 38(9): 1138-1143
- Tianjin Journal of Traditional Chinese Medicine, 2021, 38(9): 1138-1143
- http://dx.doi.org/10.11656/j.issn.1672-1519.2021.09.11
-
文章历史
- 收稿日期: 2021-04-10




2. 国家中医针灸临床医学研究中心, 天津 300381;
3. 天津市红桥区西于庄街卫生服务中心, 天津 300100;
4. 天津泰达国际心血管医院内科, 天津 300457
慢性萎缩性胃炎是消化科常见及多发的消化系统疑难疾病,也是公认的癌前病变,其患病原因较为复杂,其中幽门螺杆菌(HP)感染是引起萎缩性胃炎以及发生恶变的重要原因,以反酸、烧心、胃脘部疼痛等症状为主要临床表现,病理改变以胃黏膜上皮变薄和腺体萎缩为主,应及时进行合理干预,否则可引起贫血、胃出血及肠型胃癌前病变等并发症,本病常反复发作、迁延难愈,成为消化内科医生面对的棘手问题[1-3]。目前,临床西医常采用抗HP、保护胃黏膜等方式治疗HP感染阳性的慢性萎缩性胃炎,一定程度上能有效改善消化道不适症状,并能逆转胃黏膜病变,但整体疗效仍然不佳,且HP对抗生素极易产生耐药[4],仍需进一步优化。近年研究发现,慢性萎缩性胃炎是一种免疫系统紊乱为主导致的免疫性疾病,持续的HP感染会引起炎症免疫反应,释放大量炎症细胞因子,导致胃黏膜损伤[5];胃蛋白酶原分泌不足是引起慢性萎缩性胃炎反酸、烧心等症状的重要原因[6];胃肠激素对胃肠运动有重要的调节作用,胃肠激素表达异常是导致腹胀,腹痛,纳差等症状的重要原因[7]。慢性萎缩性胃炎属于中医胃痛、痞满范畴,采用中医药治疗不仅能够有效缓解临床症状,而且有效改善胃黏膜萎缩,阻断萎缩性胃炎发展成为胃癌的过程,全面调理整体情况,在慢性萎缩性胃炎治疗方面具有良好前景[8]。本研究旨在探讨荜铃胃痛颗粒联合三联疗法治疗慢性萎缩性胃炎合并HP感染的临床疗效及对血清胃蛋白酶原、炎症因子、胃肠激素及免疫功能的影响,现报告如下。
1 资料与方法 1.1 一般资料选择2018年12月—2020年6月收治的64例慢性萎缩性胃炎合并HP感染患者作为研究对象,将患者按随机数字表分为对照组和观察组,每组各32例,对照组中男18例、女14例;年龄为45~70岁,平均为(53.4±6.8)岁;病程为0.5~13年,平均为(4.4±2.0)年;胃镜下黏膜萎缩分级:0级7例、1级18例、2级7例;黏膜萎缩病理分级:轻度14例、中度10例、重度8例。观察组中男19例、女13例;年龄为44~70岁,平均为(53.8±6.6)岁;病程为0.5~12年,平均为(4.3±2.2)年;胃镜下黏膜萎缩分级:0级8例、1级18例、2级6例;黏膜萎缩病理分级:轻度15例、中度9例、重度8例。两组患者一般资料差异无统计学意义(P > 0.05),具有可比性。
1.2 病例入选标准 1.2.1 纳入标准1)符合萎缩性胃炎的诊断标准[8],经胃镜或黏膜活检组织病理学检查确诊。2)中医辨证为慢性萎缩性胃炎气滞血瘀证。3)13C呼吸试验结果为HP阳性。4)患者知情同意。
1.2.2 排除标准1)胃肠道癌变或先天性疾病。2)合并消化性溃疡者。3)合并精神类疾病者。4)入组前3个月内曾使用过抑酸、抗HP或胃黏膜保护药。
1.3 方法两组患者治疗期间均禁食刺激性食物,禁烟戒酒,保证充分休息。对照组患者给予标准三联方案,即雷贝拉唑(每次20 mg,每日2次)、克拉霉素(每次500 mg/次,每日2次)、替硝唑(每次5 mg,每日2次)治疗,观察组在对照组的基础上再口服荜铃胃痛颗粒,每次5 g,每日3次,两组均治疗2周。根据患者病情恢复状况和自身素质调整药物剂量。
1.4 观察指标1)治疗前及治疗2周结束时进行临床症状(纳差、呃逆、上腹部胀满、吞酸嗳气、上腹痛)评分,根据症状严重程度由轻到重分别计分为1、2、3分,评分越高表示症状越严重。2)治疗前及治疗2周结束时采用13C呼气试验检测HP根除情况,比较两组患者治疗前后HP阳性率差异。3)治疗前及治疗2周结束时进行电子胃镜检查,同时进行胃黏膜病理检查,按照文献标准[6, 9]进行炎症反应、炎症活动度、胃黏膜萎缩、肠上皮化生评分,按照指标由无到重分别计分为0~3分。4)治疗前及治疗2周结束时抽取空腹静脉血,离心分离血清,采用乳胶增强免疫比浊法检测胃蛋白酶原Ⅰ(PGⅠ)、胃蛋白酶原Ⅱ(PGⅡ),试剂盒购自北京美康生物技术研究中心,采用放免法检测胃肠激素[胃泌素(GAS)、胃动素(MTL)、生长抑素(SS)],采用酶联免疫吸附(ELISA)方法检测血清炎症因子[白介素-6(IL-6)、肿瘤坏死因子-α(TNF-α)],采用流式细胞仪检测T淋巴细胞亚群(CD4+、CD8+、CD4+/CD8+)。5)记录不良反应发生情况,记录腹泻、恶心、头痛等不良反应发生情况。
1.5 统计学方法采用SPSS 24.0统计分析软件,计数资料以构成比或率表示,组间比较采用χ2分析,计量资料以均数±标准差(x±s)表示,组内前后比较采用配对t检验,组间比较采用两独立样本t检验,P < 0.05为差异有统计学意义。
2 结果 2.1 两组患者治疗前后临床症状评分比较对照组和观察组治疗2周结束时纳差、呃逆、上腹部胀满、吞酸嗳气、上腹痛评分均较治疗前明显降低,差异具有统计学意义(P < 0.05);观察组治疗2周结束时纳差、呃逆、上腹部胀满、吞酸嗳气、上腹痛评分明显低于对照组,差异具有统计学意义(P < 0.05)。见表 1。

|
观察组治疗2周结束时HP阳性率为9.38%(3/32),对照组为37.5%(12/32),差异具有统计学意义(P < 0.05)。
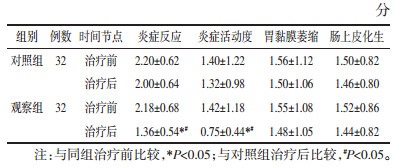
2.3 两组患者治疗前后胃黏膜病变程度及病理分级比较观察组治疗2周结束时炎症反应、炎症活动度评分均较治疗前明显降低,明显低于对照组,差异均具有统计学意义(P < 0.05),见表 2。
|
对照组和观察组治疗2周结束时PGⅠ、PGⅡ、MTL、SS较治疗前明显升高,差异具有统计学意义(P < 0.05);GAS较治疗前明显降低,差异具有统计学意义(P < 0.05);观察组治疗2周结束时PGⅠ、PGⅡ、MTL、SS明显高于对照组,差异具有统计学意义(P < 0.05);GAS明显低于对照组,差异具有统计学意义(P < 0.05)。见表 3。

|
对照组和观察组治疗2周结束时IL-6、TNF-α、CD8+较治疗前明显降低,差异具有统计学意义(P < 0.05);CD4+、CD4+/CD8+较治疗前明显升高,差异具有统计学意义(P < 0.05)。观察组治疗2周结束时IL- 6、TNF-α、CD8+明显低于对照组,差异具有统计学意义(P < 0.05);CD4+、CD4+/CD8+明显高于对照组,差异具有统计学意义(P < 0.05)。见表 4。

|
两组患者治疗过程未见严重药物不良反应,主要是皮疹、腹泻、头晕,对照组皮疹1例、腹泻1例、头晕1例,不良反应发生率为9.38%;观察组皮疹0例、腹泻0例、头晕1例,不良反应发生率为3.13%,两组不良反应发生率差异无统计学意义(P > 0.05)。
3 讨论慢性萎缩性胃炎是慢性胃炎的一种特殊类型,患者胃黏膜出现局限性或广泛性萎缩,固有腺体数量显著减少,随着病情进一步进展可出现肠上皮化生及不典型增生现象,患者对营养的吸收能力下降,可引起营养不良,导致免疫力下降,同时随着病情进展会发展为胃溃疡、胃出血等,并在胃癌的发生中起到关键性的作用,成为受医学界重视的一个疑难杂症,也越来越受到医学界的关注。慢性萎缩性胃炎病因及发病机制尚不完全阐明,与HP感染存在密切关系,采取雷贝拉唑、克拉霉素、替硝唑三联疗法对患者进行治疗,能够有效抑制胃酸分泌以及杀灭HP,但效果有限,抗菌药物耐药以及治疗方案的不规使HP根除率逐渐降低,且停药后疾病易反复发作,对预后改善造成不良影响[10-11]。
中医将慢性萎缩性胃炎归属为“胃痞”“胃脘痛”范畴,本病的发病机制主要由于外邪犯胃、内伤饮食、情志失调等因素导致胃气郁滞、脾胃升降失调而发生本病,涉及食滞、痰湿、气滞、血瘀等多方面,进而出现胃皖痞胀、疼痛、暧气、纳差、口干口苦等症状,应采取行气活血、制酸止痛为基本原则。荜铃胃痛颗粒是由荜澄茄、川楝子、醋延胡索、酒大黄、黄连、吴茱萸、醋香附、香橼、佛手、海螵蛸、煆瓦愣子等多味中药精制而成的现代中成药,其中荜澄茄、川楝子、醋延胡索为方中君药,荜澄茄温中散寒、行气止痛,具有抗菌、镇痛的药理作用,川楝子行气止痛、疏肝,具有镇痛、抗炎的药理作用,延胡索活血行气、止痛,具有镇痛、抗炎、抑制胃液分泌等药理作用,全方可起到行气活血、和胃止痛的功效,既往研究显示[12-14],荜铃胃痛颗粒治疗慢性浅表性胃炎能够有效改善胃脘痛、腹胀和反酸等症状,显著降低白介素-4(IL-4)等炎症因子水平,提高HP根除率,促进慢性胃溃疡的愈合,加快疾病康复。
本研究结果显示,观察组治疗2周结束时纳差、呃逆、上腹部胀满、吞酸嗳气、上腹痛评分均较治疗前明显降低,且明显低于对照组,观察组治疗2周结束时HP阳性率明显低于对照组组,经电子胃镜检查显示,观察组治疗2周结束时炎症反应、炎症活动度评分均较治疗前明显降低,且明显低于对照组,表明荜铃胃痛颗粒联合三联疗法治疗慢性萎缩性胃炎合并HP感染疗效显著,能够有效缓解临床症状。
胃蛋白酶主要由胃黏膜主细胞合成,是水解蛋白质的主要物质,在食物消化过程起着关键作用,并与慢性胃炎的反酸、烧心、上腹部胀满等症状相关,胃蛋白酶分泌不足使胃肠蠕动减弱,使胃内食物无法被正常消化和向后推送而腐败分解,易导致外源性酸性物质聚集和需氧菌滋生,引起消化障碍[15]。胃蛋白酶原是胃蛋白酶前身,可分为Ⅰ、Ⅱ两种类型。本研究显示,本研究结果显示,观察组治疗2周结束时PGⅠ、PGⅡ较治疗前明显升高,且明显高于对照组,表明荜铃胃痛颗粒联合三联疗法治疗慢性萎缩性胃炎合并HP感染能有效促进血清胃蛋白酶原水平,主要与其促进胃蛋白酶原的合成和分泌,同时通过抑制胃酸分泌,减少胃蛋白酶原因过量的胃酸而失活。
胃肠激素GAS、MTL、SS等指标是评估患者胃功能状态的重要指标,其中GAS具有很强的胃酸分泌作用,是评估胃黏膜固有腺体萎缩的重要标志[16];MTL的主要生理功能是影响胃肠运动,能够促进消化道平滑肌的运动,当MTL水平降低时胃黏膜局部血流量不足,可加重胃黏膜炎性病变[17];SS为抑制性胃肠激素,具有广泛的生物学效应,能够抑制胃黏膜脂质过氧化,减轻胃黏膜全层炎症,保护胃黏膜谷胱甘肽还原酶活性,从而有助于逆转逆转胃黏膜萎缩[18]。本研究结果显示,观察组治疗2周结束时MTL、SS较治疗前明显升高,且明显高于对照组,GAS较治疗前明显降低,且明显低于对照组,表明荜铃胃痛颗粒联合三联疗法治疗慢性萎缩性胃炎合并幽门螺杆菌感染能有效调节胃肠激素分泌。
HP感染后的胃黏膜会产生大量炎症因子,导致胃黏膜的炎症反应,引起胃黏膜损伤,当胃酸分泌增多时可进一步加重对胃黏膜的损伤[19-20]。本研究结果显示,观察组治疗2周结束时IL-6、TNF-α较治疗前明显降低,且明显低于对照组,表明荜铃胃痛颗粒联合三联疗法治疗慢性萎缩性胃炎合并HP感染能够有效减轻黏膜炎症反应。
慢性萎缩性胃炎存在一定程度免疫功能紊乱,对疾病良好转归造成不良影响。本研究结果显示,观察组治疗2周结束时CD8+较治疗前明显降低,且明显低于对照组,CD4+、CD4+/CD8+较治疗前明显升高,且明显高于对照组,表明荜铃胃痛颗粒联合三联疗法治疗慢性萎缩性胃炎合并HP感染能有效改善机体免疫功能,对于预防疾病复发具有重要意义。
综上所述,荜铃胃痛颗粒联合三联疗法治疗慢性萎缩性胃炎合并幽门螺杆菌感染疗效显著,能够提高HP根除率,有效调节胃肠激素分泌,促进胃蛋白酶原合成,抑制炎症反应,提高患者免疫功能,多途径共同作用促进疾病康复。
| [1] |
LI Y, XIA R, ZHANG B, et al. Chronic atrophic gastritis: a review[J]. Journal of Environmental Pathology Toxicology and Oncology, 2018, 37(3): 241-259. DOI:10.1615/JEnvironPatholToxicolOncol.2018026839 |
| [2] |
王暖凤, 初海坤, 黄树民, 等. 慢性萎缩性胃炎患者临床流行病学分析[J]. 中国公共卫生, 2017, 33(7): 1109-1111. WANG N F, CHU H K, HUANG S M, et al. Clinical characteristics of chronic atrophic gastritis patients in Heilongjiang province[J]. Chinese Journal of Public Health, 2017, 33(7): 1109-1111. |
| [3] |
郑连鹏, 马骏, 王天雄, 等. 老年慢性萎缩性胃炎与幽门螺旋杆菌感染研究[J]. 中国城乡企业卫生, 2019, 211(5): 116-117. ZHENG L P, MA J, WANG T X, et al. Study on chronic atrophic gastritis and Helicobacter pylori infection in the elderly[J]. China Urban and Rural Enterprise Health, 2019, 211(5): 116-117. |
| [4] |
白改艳, 李岩. 幽门螺杆菌耐药性机制及中药治疗进展[J]. 中国中西医结合消化杂志, 2020, 28(6): 79-83. BAI G Y, LI Y. The resistance mechanism of helicobacter pylori and the progress of traditional Chinese medicine treatment[J]. Chinese Journal of Integrated Traditional and Western Medicine on Digestion, 2020, 28(6): 79-83. |
| [5] |
宋广艳. 幽门螺杆菌感染致炎症微环境改变在萎缩性胃炎及胃癌中作用的研究[D]. 济南: 山东大学, 2013. SONG G Y. The role of helicobacter pylori infection-induced inflammatory microenvironment changes in atrophic gastritis and gastric cancer[D]. Jinan: Shandong University, 2013. |
| [6] |
汤茵, 钟碧莹, 林江英. 胃蛋白酶原在慢性萎缩性胃炎诊断中的应用价值[J]. 中国实验诊断学, 2018, 22(1): 21-24. TANG Y, ZHONG B Y, LIN J Y. Application value of Pepsinogen in patients with atrophic gastritis[J]. Chinese Journal of Laboratory Diagnosis, 2018, 22(1): 21-24. DOI:10.3969/j.issn.1007-4287.2018.01.008 |
| [7] |
史淋峰, 朱萱萱. 中医药治疗慢性萎缩性胃炎中对胃肠激素调节的研究进展[J]. 中华中医药学刊, 2011, 29(10): 2242-2246. SHI L F, ZHU X X. Traditional Chinese medicine to adjust gastrointestinal hormones in chronic atrophic gastritis[J]. Chinese Archives of Traditional Chinese Medicine, 2011, 29(10): 2242-2246. |
| [8] |
中华医学会, 中华医学会杂志社, 中华医学会消化病学分会, 等. 慢性胃炎基层诊疗指南(实践版·2019)[J]. 中华全科医师杂志, 2020, 19(9): 776-782. Chinese Medical Association, Chinese Medical Association Journal, Chinese Medical Association Gastroenterology Branch, et al. Gudieline for primary care of chronic gastritis: practice version(2019)[J]. Chinese Journal of General Practitioners, 2020, 19(9): 776-782. DOI:10.3760/cma.j.cn114798-20200706-00786 |
| [9] |
王雪华, 曹燕, 张剑宏, 等. 血清胃蛋白酶原联合胃泌素测定在胃癌及萎缩性胃炎中的诊断价值[J]. 中华临床医师杂志: 电子版, 2015, 9(10): 62-65. WANG X H, CAO Y, ZHANG J H, et al. The value of the detection of pepsinogen and gastrin levels in gastric cancer and atrophic gastritis[J]. Chinese Journal of Clinicians(Electronic Edition), 2015, 9(10): 62-65. DOI:10.3877/cma.j.issn.1674-0785.2015.10.016 |
| [10] |
高阳, 张建广, 邵佩, 等. 老年人幽门螺杆菌对抗菌药物的耐药性研究[J]. 国际老年医学杂志, 2020, 41(3): 137-140. GAO Y, ZHANG J G, SHAO P, et al. Antibiotic resistance of helicobacter pylori in older patients[J]. International Journal of Geriatrics, 2020, 41(3): 137-140. |
| [11] |
索日娜, 赵丽萍. 难治性胃炎患者幽门螺旋杆菌耐药性分析[J]. 解放军预防医学杂志, 2017, 35(2): 162-164, 167. SUO R N, ZHAO L P. Analysis of drug resistance of helicobacter pylori in patients with refractory gastritis[J]. Journal of Preventive Medicine of Chinese People's, 2017, 35(2): 162-164, 167. |
| [12] |
崔丹阳, 巩阳. 对比观察荜铃胃痛颗粒与气滞胃痛颗粒对肝胃不和型非萎缩性胃炎的临床疗效和起效时间[J]. 中华消化杂志, 2019, 39(6): 412-414. CUI D Y, GONG Y. Comparative observation of the clinical efficacy and onset time of Biling Weitong Granules and Qizhi Weitong Granules on liver-stomach discord non-atrophic gastritis[J]. Chinese Journal of Digestion, 2019, 39(6): 412-414. DOI:10.3760/cma.j.issn.0254-1432.2019.06.015 |
| [13] |
戴硙, 姚玉玲, 周莹乔. 荜铃胃痛颗粒联合兰索拉唑四联方案治疗慢性胃炎合并幽门螺杆菌感染患者的疗效研究[J]. 现代消化及介入诊疗, 2020, 25(4): 515-517. DAI Y, YAO Y L, ZHOU Y Q. The efficacy of Biling Weitong Granules combined with lansoprazole quadruple regimen in the treatment of patients with chronic gastritis complicated with helicobacter pylori infection[J]. Modern Digestion & Intervention, 2020, 25(4): 515-517. DOI:10.3969/j.issn.1672-2159.2020.04.022 |
| [14] |
高雯聪, 王永林. 荜铃胃痛颗粒联合兰索拉唑治疗慢性浅表性胃炎的临床研究[J]. 现代药物与临床, 2018, 33(12): 100-103. GAO W C, WANG Y L. Clinical study on Biling Weitong Granules combined with lansoprazole in treatment of chronic superficial gastritis[J]. Drugs & Clinics, 2018, 33(12): 100-103. |
| [15] |
孟丽英. 萎缩性胃炎患者血清胃泌素-17及胃蛋白酶原水平检测及临床意义[J]. 山西医药杂志, 2018, 47(22): 2694-2696. MENG L Y. Detection and clinical significance of serum gastrin-17 and pepsinogen levels in patients with atrophic gastritis[J]. Shanxi Medical Journal, 2018, 47(22): 2694-2696. DOI:10.3969/j.issn.0253-9926.2018.22.022 |
| [16] |
李峰, 吴焕淦, 刘雅楠, 等. 从胃泌素角度探讨针灸治疗慢性萎缩性胃炎的双向调节作用[J]. 中医学, 2019, 8(5): 301-307. LI F, WU H G, LIU Y N, et al. Discussion from gastrin on bidirectional regulating effect of acupuncture and moxibustion on chronic atrophic gastritis[J]. Traditional Chinese Medicine, 2019, 8(5): 301-307. |
| [17] |
王杰, 盛权, 朱虹, 等. 健脾益胃汤对慢性萎缩性胃炎模型大鼠血清胃泌素和血浆胃动素的影响[J]. 江苏中医药, 2014, 46(2): 77-79. WANG J, SHENG Q, ZHU H, et al. Effects of Jianpi Yiwei Decoction on serum gastrin and plasma motilin in rats with chronic atrophic gastritis[J]. Jiangsu Journal of Traditional Chinese Medicine, 2014, 46(2): 77-79. |
| [18] |
张建强, 康美清. 慢性萎缩性胃炎黏膜中胃泌素、生长抑素与脾胃虚弱证的相关性研究[J]. 中国中医急症, 2010, 19(5): 786-787, 799. ZHANG J Q, KANG M Q. Correlative study on the type of spleen-stomach weakness and GAS, SS in gastric mucosa of chronic atrophy gastritis[J]. Journal of Emergency in Traditional Chinese Medicine, 2010, 19(5): 786-787, 799. DOI:10.3969/j.issn.1004-745X.2010.05.038 |
| [19] |
张春铭. 益气活血汤治疗慢性萎缩性胃炎伴肠上皮化生的临床疗效及机制研究[J]. 四川中医, 2020, 38(2): 102-105. ZHANG C M. Clinical efficacy and mechanism of using Yiqi Huoxue Decoction in the treatment of CAG accompanied with intestinal metaplasia[J]. Journal of Sichuan Traditional Chinese Medicine, 2020, 38(2): 102-105. |
| [20] |
张海莲, 朱云, 张琦, 等. 慢性胃炎CD4+T、CD8+T细胞及Foxp3的表达及意义[J]. 蚌埠医学院学报, 2018, 43(9): 1147-1150, 1153. ZHANG H L, ZHU Y, ZHANG Q, et al. Expression and significance of CD4+T cells, CD8+T cells and Foxp3 in patients with chronic gastritis[J]. Journal of Bengbu Medical College, 2018, 43(9): 1147-1150, 1153. |
2. National Clinical Research Center for Chinese Medicine Acupuncture and Moxibustion, Tianjin 300381, China;
3. Xiyuzhuang Street Health Service Center of Hongqiao District in Tianjin, Tianjin 300100, China;
4. Department of Internal Medicine, TEDA International Cardiovascular Hospital, Tianjin 300457, China