 2022, Vol. 39
2022, Vol. 39文章信息
- 荆警提, 周锦, 张鑫, 姜皓铭, 赵志恒, 张霖, 王志强, 刘德华, 张卫红, 张军波
- JING Jingti, ZHOU Jin, ZHANG Xin, JIANG Haoming, ZHAO Zhiheng, ZHANG Lin, WANG Zhiqiang, LIU Dehua, ZHANG Weihong, ZHANG Junbo
- 基于"虚、瘀"理论探讨补肾活血法治疗Ⅱ型骨质疏松性髋部骨折的临床研究
- Based on the theory of "deficiency and stasis" to explore the clinical study of tonifying kidney and activating blood circulation in the treatment of type Ⅱ osteoporotic hip fracture
- 天津中医药, 2022, 39(9): 1118-1122
- Tianjin Journal of Traditional Chinese Medicine, 2022, 39(9): 1118-1122
- http://dx.doi.org/10.11656/j.issn.1672-1519.2022.09.09
-
文章历史
- 收稿日期: 2022-03-15





2. 深圳市罗湖区中医院骨伤科,深圳 518001;
3. 天津中医药大学第二附属医院脑病针灸中心,天津 300250
骨质疏松是一种以骨量减低、骨组织微结构损坏,导致骨脆性增加、易发生骨折为特征的全身性骨病,随着年龄增长发病率增高[1-2]。Ⅱ型骨质疏松即老年骨质疏松,其病理特征表现为骨小梁变细且数量减少、骨小梁间隙增宽。Ⅱ型骨质疏松髋部骨折在临床中很常见,据推测分析,至2050年,中国Ⅱ型骨质疏松性髋部骨折患者将达599万例,已成为中国面临的重要公共卫生问题[3-4]。对于老年骨质疏松性髋部骨折患者多建议手术治疗,尽早恢复下地活动[5-6]。本研究依据“虚、瘀”理论,采用补肾活血法辨证治疗Ⅱ型骨质疏松性髋部骨折,深入研究其临床效果,现报道如下。
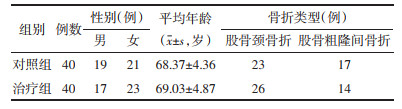
1 资料与方法 1.1 一般资料2020年6月—2021年3月,纳入本院骨伤科收治的单侧股骨颈或股骨粗隆间新鲜闭合骨折行内固定治疗的老年患者80例。采用随机数表法将患者随机分为治疗组和对照组,每组40例,两组患者一般资料比较,差异均无统计学意义,具有可比性。见表 1。
参照《中国骨质疏松性骨折诊疗指南(骨质疏松性骨折诊断及治疗原则)》[7]和《实用骨科学》(2016年版)[8]有关股骨颈和股骨粗隆间骨折的诊断标准:1)平素骨痛或有脆性骨折史,骨密度(BMD):< -2.5SD(双能X线骨密度测量仪测定)。2)有明确的外伤史。3)伤肢轴向叩击痛,腹股沟区压痛或大转子部叩击痛,伤肢外旋、短缩、轻度屈曲畸形。4)影像学可明确骨折类型及移位程度。
1.2.2 中医诊断标准依据《中医病证诊断疗效标准》[9]和《中药新药临床研究指导原则》[10]制定肝肾亏虚兼血瘀证型辨证标准:腰背酸软隐痛、下肢痿软无力、持重困难,髋部青紫肿胀、刺痛、局部瘀斑,舌红或紫伴有斑点、脉弦细。
1.3 病例筛选标准 1.3.1 纳入标准1)符合上述诊断标准。2)年龄在65~80岁之间。3)根据影像学及患者身体状况,可耐受手术,且内固定术能提供坚强固定。4)自愿参加并签署知情同意书。
1.3.2 排除标准1)不符合诊断和纳入标准。2)陈旧性骨折或骨折伴有髋关节疾病。3)半年内曾使用过影响骨代谢药物者。4)患有严重心脑血管疾病、肝肾等疾病。5)患有引起继发性骨质疏松症的疾病。6)围手术期出现严重并发症需要治疗者。7)拒服中药或服用中药不适者。8)难以配合完成研究者。
1.3.3 剔除标准1) 出现严重不良事件。2)试验过程中出现严重的合并疾病。3)患者自行退出研究。
1.4 治疗方法两组手术由同一组医师完成,股骨颈骨折采用空心螺钉内固定术或动力髋螺钉(DHS)内固定术。股骨粗隆间骨折采用防旋股骨近端髓内钉(PFNA)内固定术,两组患者予同样的常规治疗。术后第1天开始口服中药,两组中药用法:150 mL,早晚各1次,饭后温服。两组疗程均为6个月。
治疗组予强骨活血汤(当归15 g,熟地黄30 g,红花10 g,桃仁10 g,川芎10 g,赤芍10 g,黄芪30 g,续断10 g,骨碎补15 g,补骨脂10 g,牛膝10 g,香附10 g,土鳖虫10 g,炙甘草10 g)。
对照组按3期辨证用药(均来自《中医骨伤科学》),术后1~2周予活血祛瘀汤(当归15 g,红花6 g,土鳖虫9 g,自然铜9 g狗脊9 g,骨碎补15 g,没药6 g,乳香6 g,三七3 g,路路通6 g,桃仁9 g);3~6周予新伤续断汤(当归尾12 g,
两组患者术前、术后1~6个月拍摄髋部X线片评估骨折愈合情况,术后3个月、6个月检查L1-4和健侧股骨颈骨密度,晨起空腹抽静脉血检查T-PINP、β-CTX、N-MID指标。术后6个月评估髋关节功能、生活质量水平。
1.5.1 骨折临床愈合标准采用《中医骨伤科学》[11]中的骨折临床愈合标准。
1.5.2 Harris髋关节功能评分包含4部分:疼痛(44分),功能(47分),畸形(4分),活动度(5分),共100分。分4个级别:优(90~100分),良(80~89分),可(70~79分),差(小于70分)[12]。
1.5.3 生活质量评估欧洲五维健康量表[13]是一种多维健康相关生存质量量表,包含健康描述系统(EQ-5D)和刻度尺(EQ-VAS)两个部分,EQ-5D包括5个项目:疼痛或不舒服、行动能力、日常活动能力、自己照顾自己能力、焦虑或抑郁。每个项目包含:无困难(1分)、有些困难(2分)、极度困难(3分)。通过公式计算EQ-5D指数得分。EQ-VAS是1个长20 cm的视觉刻度尺,患者依据自身当天感受为自己健康状态打分,100分表示“最好的健康状况”,0分表示“最差的健康状况”。
1.6 统计学方法采集数据建立Excel数据库,选用SPSS 22.0软件进行数据统计分析,符合正态分布的计量资料以均值±标准差(x±s)表示,组内重复测量的试验数据采用重复测量方差分析,组间比较采用两独立样本t检验。计数资料用例数及构成比表示,组间比较采用χ2检验。P<0.05为差异有统计学意义。
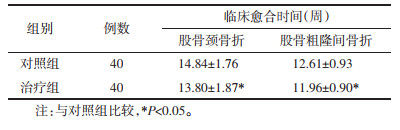
2 结果 2.1 两组患者骨折临床愈合时间比较治疗组骨折临床愈合时间较对照组缩短,差异有统计学意义(P < 0.05),见表 2。
|
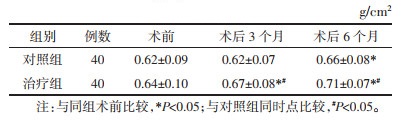
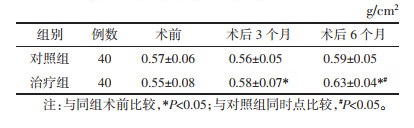
对照组患者L1-4骨密度术后6个月与术前比较,差异有统计学意义(P < 0.05);治疗组患者L1-4骨密度术后3个月和6个月,与同组术前比较,差异有统计学意义(P < 0.05)。治疗组患者术后3个月和6个月L1-4骨密度与对照组比较,差异有统计学意义(P < 0.05)。治疗组患者术后3个月和6个月健侧股骨颈骨密度与术前比较,差异有统计学意义(P < 0.05);术后6个月,治疗组与对照组比较,差异有统计学意义(P < 0.05)。见表 3和表 4。
|
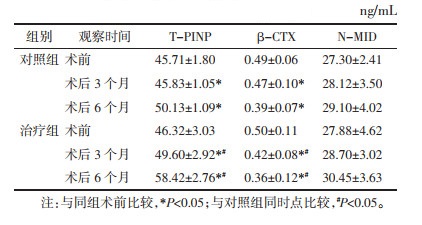
对照组和治疗组术后3个月和术后6个月T-PINP、β-CTX与同组术前比较,差异有统计学意义(P < 0.05),N-MID与同组术前比较,差异无统计学意义(P>0.05);治疗组术后3个月和术后6个月T-PINP、β-CTX与对照组比较,差异有统计学意义(P < 0.05)。N-MID与对照组比较差异无统计学意义(P>0.05)。见表 5。
|
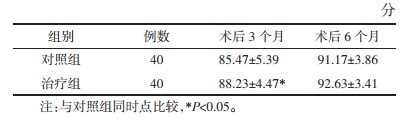
术后3个月,治疗组Harris髋关节功能评分明显优于对照组,差异有统计学意义(P < 0.05),术后6个月,两组患者Harris髋关节功能评分,差异无统计学意义(P>0.05)。见表 6。
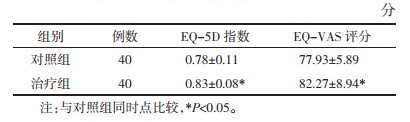
治疗组生活质量水平EQ-5D指数、EQ-VAS评分均优于对照组,差异均有统计学意义(P < 0.05)。见表 7。
|
对照组1例患者发生左下肢肌间静脉血栓,按体质量予低分子肝素抗血栓治疗2周后复查下肢动静脉彩超血栓消失。两组患者均有1例口服中药后胃部不适,予口服艾司奥美拉唑镁肠溶片后胃部不适症状消失。
3 讨论本研究选用深圳市罗湖区人民医院骨伤科自拟强骨活血汤治疗老年骨质疏松性髋部骨折,方中首选熟地黄滋补肾阴、填精益髓,当归补血活血,两者合用,补而不滞,活血而不伤正,共为君药。臣以红花、桃仁、川芎、赤芍助君药活血行气,祛瘀止痛。黄芪健脾补气,助当归补气生血,充养肾中先天之精。佐以牛膝补肝肾强筋骨,同时引血下行;续断、骨碎补、补骨脂增强补肾强骨、活血通络之效,同时有续筋接骨疗伤之功;香附理气止痛,土鳖虫活血通瘀。炙甘草益气补中,缓急止痛,又可缓和药性为使药。现代药理研究表明,熟地黄主要活性成分是苯乙醇苷类、环烯醚萜苷类,可促进成骨细胞形成[14-15]。当归、川芎中主要活性成分为藁本内酯,其通过GPR30/EGFR途径调控成骨细胞的存活和凋亡,显著增多成骨细胞的数量[16]。Wang等[17]研究证实藁本内酯通过NF-κB/ERK/p38/ITAM信号通路抑制RANKL表达,从而影响破骨细胞的活性和分化。研究表明,骨质疏松性骨折患者应用桃仁、红花,能有效改善骨折局部微循环,从而增加血供促进骨折修复[18]。黄芪的有效成分黄芪多糖可促进成骨细胞的增殖,通过抗氧化应激作用治疗骨质疏松[19]。骨碎补总黄酮有类雌激素作用,对雌激素降低形成的骨质疏松有良好的效果,体外细胞实验也证明了骨碎补总黄酮可以通过多信号通路促进成骨细胞的分化和成熟,同时可抑制破骨细胞的活化,可有效治疗骨质疏松症[20]。
本研究结果显示,术后6个月,两组患者L1-4和股骨颈骨密度明显优于术前(P < 0.05),并且治疗组明显优于对照组,差异有统计学意义(P < 0.05),说明两组治疗均能够提高骨密度,改善骨质疏松状况,但治疗组方案更优。两组患者骨密度的改善也与健康教育、调整生活模式、功能锻炼指导等有一定的关系。术后3个月和6个月,治疗组T-PINP均高于对照组(P < 0.05),β-CTX均低于对照组(P < 0.05),说明治疗组方案能够调控骨转换标志物,抗骨吸收并促进骨形成,N-MID变化不明显(P>0.05),可能与老年人低代谢水平有关。治疗组骨折临床愈合时间较对照组缩短,差异有统计学意义(P < 0.05)。术后3个月,治疗组Harris评分明显优于对照组(P < 0.05),术后6个月,两组患者Harris评分差异无统计学意义(P>0.05),说明治疗组方案能够促进髋部骨折术后早期康复。术后6个月治疗组生活质量水平EQ-5D指数、EQ-VAS评分均优于对照组(P < 0.05),说明治疗组方案能够有效提高髋部骨折术后生活质量。
研究显示补肾活血法可促进Ⅱ型骨质疏松性髋部骨折愈合,提高骨密度,改善骨代谢,并提高患者术后生活质量水平。
| [1] |
BIJLSMA A Y, MESKERS C G M, WESTENDORP R G J, et al. Chronology of age-related disease definitions: Osteoporosis and sarcopenia[J]. Ageing Research Reviews, 2012, 11(2): 320-324. DOI:10.1016/j.arr.2012.01.001 |
| [2] |
SERIOLO B, PAOLINO S, CASABELLA A, et al. Osteoporosis in the elderly[J]. Aging Clinical and Experimental Research, 2013, 25(1): 27-29. |
| [3] |
贺丽英, 孙蕴, 要文娟, 等. 2010—2016年中国老年人骨质疏松症患病率Meta分析[J]. 中国骨质疏松杂志, 2016, 22(12): 1590-1596. HE L Y, SUN Y, YAO W J, et al. The prevalence rate of osteoporosis in the elderly in China from 2010-2016:a Metaanalysis of single rate[J]. Chinese Journal of Osteoporosis, 2016, 22(12): 1590-1596. DOI:10.3969/j.issn.1006-7108.2016.12.019 |
| [4] |
SI L, WINZENBERG T M, JIANG Q, et al. Projection of osteoporosis-related fractures and costs in China : 2010-2050[J]. Osteoporosis International, 2015, 26(7): 1929-1937. DOI:10.1007/s00198-015-3093-2 |
| [5] |
张培训, 许庭珉. 老年骨质疏松性髋部骨折的围术期处理策略[J]. 中国骨与关节杂志, 2020, 9(6): 401-403. ZHANG P X, XU T M. Perioperative management of senile osteoporotic hip fracture[J]. Chinese Journal of Bone and Joint, 2020, 9(6): 401-403. DOI:10.3969/j.issn.2095-252X.2020.06.001 |
| [6] |
虞宵, 郭东昇, 周晓强, 等. 老年骨质疏松髋部骨折中ERAS规范化诊疗的临床应用[J]. 南京医科大学学报(自然科学版), 2020, 40(3): 426-430. YU X, GUO D S, ZHOU X Q, et al. Clinical application of ERAS standardized diagnosis and treatment in senile osteoporotic hip fracture[J]. Journal of Nanjing Medical University (Natural Sciences), 2020, 40(3): 426-430. |
| [7] |
邱贵兴, 裴福兴, 胡侦明, 等. 中国骨质疏松性骨折诊疗指南(全文)(骨质疏松性骨折诊断及治疗原则)[J]. 中华关节外科杂志(电子版), 2015, 9(6): 795-798. QIU G X, PEI F X, HU Z M, et al. Chinese guidelines for diagnosis and treatment of osteoporotic fractures (full text) (principles of diagnosis and treatment of osteoporotic fractures)[J]. Chinese Journal of Joint Surgery (Electronic Edition), 2015, 9(6): 795-798. DOI:10.3877/cma.j.issn.1674-134X.2015.06.021 |
| [8] |
田伟, 王满宜, 郭源, 等. 实用骨科学[M]. 北京: 人民卫生出版社, 2016: 502. TIAN W, WANG M Y, GUO Y, et al. Practice of orthopaedics[M]. Beijing: People's Medical Publishing House, 2016: 502. |
| [9] |
国家中医药管理局. 中医病症指导疗效标准[M]. 南京: 南京大学出版社, 2012: 186. National Administration of Traditional Chinese Medicine. Traditional Chinese medicine Syndrome diagnostic efficacy of standard[M]. Nanjing: Nanjing University Press, 2012: 186. |
| [10] |
郑筱萸. 中药新药临床研究指导原则[M]. 北京: 中国医药科技出版社, 2002: 357. ZHENG X Y. Guidelines for clinical research of traditional Chinese drug research[M]. Beijing: China Medical Science Press, 2002: 357. |
| [11] |
王和鸣. 中医骨伤科学[M]. 2版. 北京: 中国中医药出版社, 2007: 132. WANG H M. Traditional Chinese orthopedics[M]. 2nd ed. Beijing: China Press of Traditional Chinese Medicine, 2007: 132. |
| [12] |
SUAREZ-AHEDO C, GUI C C, RABE S M, et al. Relationship between age at onset of symptoms and intraoperative findings in hip arthroscopic surgery[J]. Orthopaedic Journal of Sports Medicine, 2017, 5(11): 2325967117737480. |
| [13] |
骆洪涛, 郑力通, 闫伟, 等. 欧洲五维健康量表评估老年髋部骨折术后生活质量变化的研究[J]. 中华关节外科杂志(电子版), 2015, 9(2): 200-204. LUO H T, ZHNEG L T, YAN W, et al. Europe quality of life assesses life quality of elderly patients after hip surgery[J]. Chinese Journal of Joint Surgery (Electronic Edition), 2015, 9(2): 200-204. DOI:10.3877/cma.j.issn.1674-134X.2015.02.011 |
| [14] |
张乃丹. 基于分子对接策略的熟地黄防治糖尿病性骨质疏松症有效成分及其作用机制研究[D]. 上海: 第二军医大学, 2016. ZHANG N D. Studies on chemical constituents and mechanism of Rehmanniae Radix Preparata for diabetic osteoporosis based on molecular docking strategy[D]. Shanghai: Second Military Medical University, 2016. |
| [15] |
LIU C Y, MA R F, WANG L L, et al. Rehmanniae Radix in osteoporosis: a review of traditional Chinese medicinal uses, phytochemistry, pharmacokinetics and pharmacology[J]. Journal of Ethnopharmacology, 2017, 198: 351-362. DOI:10.1016/j.jep.2017.01.021 |
| [16] |
YANG F, LIN Z W, HUANG T Y, et al. Ligustilide, a major bioactive component of Angelica sinensis, promotes bone formation via the GPR30/EGFR pathway[J]. Scientific Reports, 2019, 9: 6991. DOI:10.1038/s41598-019-43518-7 |
| [17] |
WANG D R, LI J, FENG W Y, et al. Ligustilide suppresses RANKL-induced osteoclastogenesis and bone resorption via inhibition of RANK expression[J]. Journal of Cellular Biochemistry, 2019, 120(11): 18667-18677. DOI:10.1002/jcb.29153 |
| [18] |
曹舜, 丁洪伟. 桃仁承气汤联合唑来膦酸预防老年骨质疏松压缩骨折PVP/PKP术后新发椎体骨折疗效及对骨代谢生化指标的影响[J]. 现代中西医结合杂志, 2019, 28(7): 728-731. CAO S, DING H W. Effect of Taoren Chengqi Decoction combined with zoledronic acid on prevention of new vertebral fracture after PVP/PKP in aged osteoporotic patients and its influence on biochemical indexes of bone metabolism[J]. Modern Journal of Integrated Traditional Chinese and Western Medicine, 2019, 28(7): 728-731. DOI:10.3969/j.issn.1008-8849.2019.07.012 |
| [19] |
思志强, 张莹, 贾英杰. 中药黄芪防治骨质疏松研究进展[J]. 辽宁中医药大学学报, 2019, 21(10): 214-217. SI Z Q, ZHANG Y, JIA Y J. Advances in research on prevention and treatment of osteoporosis with Chinese medicine Astragalus[J]. Journal of Liaoning University of Traditional Chinese Medicine, 2019, 21(10): 214-217. |
| [20] |
SONG S H, ZHAI Y K, LI C Q, et al. Effects of total flavonoids from Drynariae Rhizoma prevent bone loss in vivo and in vitro[J]. Bone Reports, 2016, 5: 262-273. DOI:10.1016/j.bonr.2016.09.001 |
2. Department of Orthopaedics and Traumatology, Shenzhen Luohu District Hospital of Chinese Medicine, Shenzhen 518001, China;
3. Encephalopathy Acupuncture Center, Second Affiliated Hospital of Tianjin University of Traditional Chinese Medicine, Tianjing 300250, China